Rural urbanisation leaves trail of obesity and chronic diseases
It is estimated that by 2030, chronic pulmonary diseases will be the leading killers worldwide and villagers practise just about every lifestyle that encourages the illnesses. GRAPHIC | MILLICENT WACHIRA
What you need to know:
Westernisation in the rural areas is leaving a trail of obesity, heart diseases, diabetes, kidney failure, hypertension, cancer and deadly chronic obstructive pulmonary disease (COPD); illnesses that don’t even have names in vernacular languages.
There was a time when what was known of Kenya’s villages was malaria, hunger and infant deaths. The rural households were too poor to afford cigarettes, too hungry and hard-working to be overweight.
But now, on arrival in the mud-and-thatch villages, settlements with no running water and electricity, you would never guess that thousands of the farmers and livestock keepers who live there die from chronic diseases associated with a far more opulent Western lifestyle, says Prof Gerald Yonga, the Kenya Cardiac Society national chair.
Westernisation in the rural areas is leaving a trail of obesity, heart diseases, diabetes, kidney failure, hypertension, cancer and deadly chronic obstructive pulmonary disease (COPD); illnesses that don’t even have names in vernacular languages.
Men with carts sell sausages and home-made ice-creams sachets in trading centres. At lunchtime, young children line up to buy hot potato chips made over smoky fires, wrapped in small polythene bags.
"Traditional staples such as maize, vegetables and the occasional meat or fish that were previously steamed or boiled are now fried in saturated fat. Meals once seasoned with herbs are now heavily salted. People eat more meat, potato chips have arrived in rural shops and children are clamouring for soda," said Prof Yonga, a consultant cardiologist at Aga Khan University Hospital.
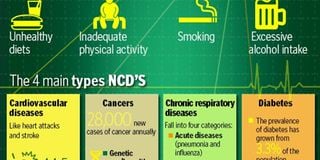
Unhealthy diets, inadequate physical activity, smoking and excessive alcohol intake have pushed up the numbers of Kenyans with obesity, high cholesterol, high blood pressure and diabetes, and the villages tucked in forests or rocks, as if shielded from affluence, are now feeling the growing pains of globalisation.
A real problem Prof Yonga says is that more and more women in rural areas are growing overweight. The irony is that Kenya has high levels of malnutrition and rising numbers of obese people.
Obesity weighs down on body joints and combined with lack of physical activity, puts people at risk of getting arthritis, heart diseases, hypertension, diabetes, cancer and obstructive lung diseases.
Nor has high blood pressure spared the poor households. According to AstraZeneca, a biopharmaceutical company, about 44.5 per cent of Kenyan adults have raised blood pressure, which is one of the highest prevalence rates across Africa. These hypertensive patients are staring at damaged hearts, arteries, brains, kidneys, eyes and sexual dysfunction.
Healthy Heart Africa, a programme launched in October last year by the UK pharmaceutical targets to train low-income populations, at-risk adults over 35 years in areas like Kajiado, Kirinyaga, Vihiga, and Nyamira on hypertension risk factors and healthy behaviours.
Physical inactivity is no longer only a problem of the affluent. Boda bodas race through the villages picking commuters to markets, dispensaries or churches. Most rural dwellers do not have to walk far, reducing their physical activity to bare minimum.
Nicotine- laden
In emerging towns, high-rise buildings are coming up, crowding the towns. "There is less space for walking. And even if you wanted to walk, there is fear of insecurity or being knocked down," Prof Yonga says.
Smoking is a big problem in rural areas. ‘‘They (rural dwellers) may not buy the Cuban cigars, the shisha or expensive cigarette brands. But they buy the cheap poor quality nicotine-laden filter-less cigarettes. Some of them farm the tobacco in a garden patch behind their huts. They dry it on the roof top and then roll it,’’ says Dr Peter Munyu, a pulmonary specialist at Aga Khan University Hospital.
Of concern to Dr Munyu is COPD, a life-threatening lung disease projected to be the third leading killer by 2030 worldwide. The disease, a persistent inflammation of the lungs’ airways, is most often caused by tobacco smoke or exposure to stove smoke.
Africa is expected to bear the brunt of the disease that interferes with breathing and is not fully reversible due to increase in smokers.
‘‘Unfortunately, new smokers are now found in developing nations like Kenya as more people in rich countries drop the habit or avoid it at all,’’ says Dr Munyu.
Experts say tobacco control laws in high-income countries are so strict that cigarette companies are expanding their markets into Africa where laws are less stringent.
‘‘Instead of having a static or reducing number of smokers in Kenya, we are seeing an increase in smokers, especially among educated women and college- going young people,’’ says Prof Yonga.
Most women in the villages also cook food using firewood, exposing themselves and their small children to smoke that damages the hearts and lungs. The men who have moved to industries and quarries are also exposed to industrial pollutants and dust.
With the majority of the men in rural areas using tobacco, COPD is likely to hit poor households harder. Of the 2.5 million Kenyan adults currently using tobacco (smoking and/or smokeless tobacco), about 12.9 per cent or 322,500 are found in rural areas, according to the Global Adult Tobacco Survey, 2014.
But Prof Yonga says Kenya could be underestimating tobacco use in rural areas. The National Authority for Campaign against Alcohol and Drug Abuse (Nacada) statistics show that the Central region leads with 22.6 per cent of the males using tobacco products. For females, Eastern region leads with 5.7 per cent of the women smoking or chewing tobacco products.
Kenya has stepped up the war on smoking with new tougher laws, but in rural areas people still smoke in public, exposing others to second-hand smoke.
In the dusty outskirts of Eldoret town, a man buys a cigarette from a vendor selling his wares under a tree. He lights it and starts smoking.
‘‘We hear there is a law banning people from smoking in public, but this is not Nairobi. We just smoke, no one stops us,’’ says a man who only gives his name as Kipchirchir.
He says he knows the risks of smoking and one day he will stop. But before he does, if he will, the tobacco smoke would have changed the way his lungs operate, paralysing cells lining the airways, making it hard for him to expel mucus effectively. The tobacco smoke will predispose him to bronchus, oesophagus, lung, lips, mouth, airway cancers among other illnesses.
Warning signs
Experts say Kenya has made modest changes in tobacco use, but still more has to done.
‘‘Advertising is subtle, labelling of cigarette packets is not as visible. But in New York, the difference is massive. Cigarette packets are filled almost completely with pictorials. If you bought the cigarette in a packet laden with warning signs, you will know what you are buying,’’ says Prof Yonga.
In Kenya, traders are still selling cigarettes in sticks instead of packets and the country lacks adequate support for those seeking to quit smoking. Dr Munyu says cessation drugs like nicotine replacement gums and sprays are expensive.
‘‘A person may use on average Sh6,000 to Sh8,000 per month for the nicotine gums or patches, plus doctor’s consultation fees. The government may need to consider reducing taxes charged on these drugs,’’ he says, adding that insurance companies should also pay for cessation sessions as some patients struggle for months before quitting, so they find it hard to pay from out of pocket.
Chronic disease are estimated to cause 30 per cent of mortality in Kenya with infectious diseases like HIV/Aids, acute respiratory tract infections and diarrhoea contributing to the majority of deaths in Kenya. But as the tide turns, the country is staring at a double burden of disease.
‘‘We are beginning to have diseases of behavioural changes while we haven’t gotten rid of the infectious diseases. We still have a lot of malaria, tuberculosis, HIV/Aids, diarrhoea, respiratory diseases as causes of mortality while we are getting new ones,’’ warns Prof Yonga.
There are concerns that the new chronic illnesses may surpass maternal, child and infectious diseases as the biggest killer in years to come. With many Kenyans living on less than a dollar a day, the costly ailments are set to strain poor households which rely on out of pocket cash to go to hospital.
‘‘The economic toll from chronic diseases is devastating to the family, and the national economy leading to billions of shillings lost due to healthcare costs and reduced productivity from the disabling and fatal outcomes related to these diseases,’’ notes Prof Yonga in a case study on chronic non-communicable diseases in Kenya.
As the chronic diseases spread fast, the country is ill-prepared. It lacks enough oncologists, cardiologists, lung, kidney and doctors. There few health facilities equipped to diagnosis these diseases early. The few doctors that are available are concentrated in Nairobi.