Time flies with great content! Renew in to keep enjoying all our premium content.
Prime
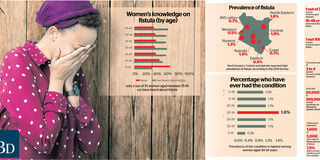
Push for safer births as fistula cases increase
BD GRAPHIC
At first glance she is happy and smiling, entering the Accident and Emergency conference room at Kenyatta National Hospital, waiting for the final press briefing to mark a successful 16-day obstetric fistula camp.
Muthoni, is lucky to be here, healthy and able to sit in a room full of people, without worrying about the smell she is emitting, or whether her clothes are messed up with urine and faeces.
She is one of 115 women who benefited from free surgery and treatment during the camp at the hospital for tweks until July 12, where 603 women from East Africa showed up for screening KNH ran in partnership with the Flying Doctors Society, UNFPA, Amref and Safaricom Foundation..
For this 35-year-old mother of two, she doesn’t take for granted things that most people would consider insignificant or mundane. For instance, being able to walk into the washroom without worrying about washing up after.
“I went for a long call normally for the first time, a few days after the surgery, without having to worry about having to wash myself up and that was more than satisfactory,” she says as she recalls the hell she has lived in for the past 13 years. It all began in 2006 after giving birth to her first born.
Throughout her pregnancy, life was normal, and like most mothers she couldn’t wait to come face to face with her bundle of joy. But the problem began after giving birth.
“I gave birth to my daughter at home with the help of a midwife,” she says. Though she had a chance to hold her bundle of joy, her happiness was cut short.
“I bled for two days and that’s when I decided to go to hospital, and that’s when they discovered that I had a tear during birth.” That was the beginning of her nightmare. “I started passing feces uncontrollably,” she says.
She ignored the whole matter, considering that at the time, she could control the situation, and never in her mind did she ever thought that it was obstetric fistula. But the worse was still to come. In November 2016, she got pregnant again.
“I never experienced any complications during the whole pregnancy period up until to the hospital experiencing labour pain."
The labour lasted three days. She remembers lying in bed unaware of the extent of the damage, until the doctor came in to check whether the cervix had dilated. “After he had inserted the fingers in the cervix to check for dilation, and found out that I had dilated for six centimetres.
Thus, I thought I could give birth normally. But then he would later reveal that I was suffering from obstetric fistula, meaning I couldn’t have a normal birth. That’s when the reality dawned,” she says.
But still, she hadn’t thought of the magnitude of the situation, only thinking of having her baby and going back home.
“This time round, I gave birth through Caesarean section, and after a few days I was allowed to go home,” she says. Still, she never imagined the miserable lifestyle that was awaiting her. The complications that she had after giving birth to her first child had gotten worse.
“This time round, the urine started mixing with faeces and leaking without my control.
During my menses, the periods would also mix with all the other waste,” she describes.
Her lifestyle took a turn for the worse. “I stopped wearing panties and instead got used to the rags to drain the mess.” That’s not just it, she was forced to be so watchful of what she ate, at what time. “I couldn’t take lots of fluids or eat soft meals, since it would mean soft poop, faeces that would come out easily, making it hard for me to control. With dry foods like bread, the faeces would be a little hardened, thus maybe give me a cue before the leak, giving me the time to rush to the toilet.”
She was confined to her home, and particularly her room from where she could clean herself up.
“My room is just next to my toilet yet it was a miracle to make it in time.” She couldn’t go for long journeys, and she recalls that even the shortest trips from her home in the outskirts of Nairobi to the central business district would require planning.
“Planning in terms of dressing, as well as a meal that I would eat the previous day,” she says, adding that on long journeys, she would be forced to put on adult diapers.
Apart from that, she was passing air uncontrollably and loudly especially while standing up after sitting for a while, an ordeal that most of the time would leave her embarrassed. “For this reason, in public transport I had to make sure that I came out last." But all these is nothing compared to the stigma she has had to undergo, especially from people she considered to be close to her.
“I’ve had people linking my condition to promiscuity.” Intimacy on the other hand, for the last three years, became a thing of the past.
“Since I got pregnant with my second child, I haven’t been intimate with anyone.” Chebet, a Bomet resident, prior to her surgery, also courtesy of the campaign, had suffered from obstetric fistula since 1993. This was after the birth of her only child, where her condition involved leaking urine. “I tried going to various hospitals without getting help, thus I had to adopt to this condition. For instance, I couldn’t go for long journeys because I had to stay close to home to wash my rugs and hang them ready for use again.
Adult diapers were out of my reach since I didn’t have a source of income.” That was not her only nightmare, since the condition also took a toll on her marriage, opting to go back to her parents three years ago.
For these two, their nightmare became a thing of the past, thanks to the obstetric fistula camp, but even as they embark on their normal life with joy, many women continue to suffer from this condition.
The World Health Organisation estimates that more than two million women live with fistula worldwide. Studies show that each year 50,000 to 100,000 women worldwide are affected by obstetric fistula.
According to data from a 2011 report by Campaign to End Fistula, there are an estimated 1,000 to 3,000 new cases of each year in Kenya, with only 7.5 percent able to access medical care. In Kenya, it is estimated that the occurrence stands at three to four women for every 1,000 deliveries, with fistula accounting for at least six percent of all maternal deaths and prenatal loss if left untreated.
Not many women are able to afford treatment. At a private hospital it would cost between Sh250,000 and Sh450,000, while in public facilities it is between Sh50,000 and Sh90,000.
Dr Khisa Wakasiaka, a gynaecologist consultant/fistula surgeon at KNH , says the problem is mostly rampant in rural areas where there are cases of unskilled birth attendants. Though he says obstruction occurs everywhere and can’t be prevented, Dr Wakasiaka insists that it should be controlled to prevent fistula.
“We cannot prevent women from getting pregnant, thus they should be able to get their babies without disabilities,” he says.
According to Dan Okoro, a reproductive health specialist, there is a need to get quality care right during pregnancy.
“Most are as a result of inappropriate care while giving birth, which should be dealt with. Even though there’s no guarantee of a free injury birth, they should not develop to disabilities,” Dr Okoro says. Dr Khisa says treatment does not involve just the physical part of it. “It also includes restoration of dignity and life for the victims, thus helping them to achieve self-confidence.”
Unlock a world of exclusive content today!Unlock a world of exclusive content today!