In the calm Katopoton village in West Pokot, Prisca Chemining goes about chores at home, but says her heart is with her children who are away in hospital under the care of her husband. She wasn’t able to take them there herself because she has also been unwell.
The children have been diagnosed with pneumonia — a potentially deadly respiratory disease that inflames the lungs, leading to painful coughs and difficulty in breathing.
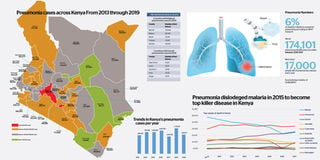
Chemining’s son is one of the 1,333,000 people that sought care for pneumonia in hospitals in Kenya in 2019 alone, according to the data from the national health information system. Majority of these were children.
While Chemining’s son survived, some die.
In 2016, the Unicef reported that there were more than 34,000 deaths due to acute respiratory infections, mostly pneumonia, 14 per cent of all the deaths of children under five.
A 2017 study by UK based organisation Save the Children, pneumonia kills two children under five every minute, an equivalent of one million a year worldwide. Majority of these deaths are in sub-Sahara Africa.
While the numbers have reduced, the disease remains Kenya’s number one child killer, and health experts have many reasons.
Researcher David Gathara, said attention has not been given to the respiratory killer even when data shows it is the greatest threat to children.
“Perhaps even more that than HIV and malaria where we all have our attention,” he says.
Pneumonia presents with a cough accompanied by short laboured breath. Many microorganisms —such as bacteria and viruses — enter the lungs and clog the air sacs with fluid. This reduces oxygen uptake that aids in breathing.
Ambrose Agweyu, a paediatrician and disease patterns and pneumonia researcher at the Kenya Medical Research Institute (Kemri) Wellcome Trust— told the Business Daily: “From prevention, to the time the mother gets to the hospital is a chain, and when it breaks anywhere, a child dies.”
This is particularly prevalent in arid and semi-arid counties in Kenya.
He said: “There are vaccines given for free to children but then there is the issue of access where mothers cannot even afford fare to the hospital.”
Kenya introduced the pneumonia vaccine in 2011 to be administered to children at weeks 6, 10 and 14. According to the Pneumococcal Conjugate Vaccine Impact Study (PCVIS) that was published in Lancet this year, children admitted to Kilifi County hospital with clinically defined pneumonia reduced by 27 percent.
Ifedayo Adetifa, a paediatrician and clinical epidemiologist who was part of the study said that before the introduction of the vaccine, the incidence of the disease was 1,220 children per 100,000 which reduced to 891.
However, in Samburu East, in Lekea village, women walk for two hours with babies strapped to the back, carrying with them food and water to take them through that rough terrain. They are seeking vaccination brought by a non-governmental organisation.
The terrain is unforgiving: the sun is hot; wild animals roam freely and there are rivers such as Lengusaka that if they are unlucky it rains, the women have to sit on the sides and wait for the water levels to drop before attempting to cross.
When the outreach camp does not come, they walk for a whole day to Suari or another eight hours to Ngilai to look for a health centre. They spend the night there and wake up the next day to return home.
Njelai, a mother of two, said at Marmarai Health Centre in East Samburu, the nearest health facility is Wamba Health Centre. That is nearly 74 kilometres away.
INDOOR POLLUTION
A nurse that runs these outreach camps, Teobalda Michaels, said she could draw a straight line between the cases of pneumonia and what the mothers used to cook for the children in the huts with poor ventilation.
Indeed, studies have shown that children in homes with indoor pollution due to the use of charcoal and wood are more likely to die of pneumonia.
Dr Agweyu said that it is suspected that the fine particles and toxic gases in cooking smoke inflame the babies’ lungs, which makes them twice as vulnerable to pneumonia
But even when the mother does overcome these challenges and go to the facility, there is no guarantee that she would find a healthcare worker in the hospital with the tools to treat the child.
When this reporter visited Obama Children’s ward in the referral hospital in Kisumu County, there were no children in the ward because the healthcare workers were on strike.
Obama Ward is an 80-bed capacity with beds specially made that the mother and the baby can sleep on the same bed without hurting the child. The ward is always 150 per cent full at any given time.
Senior nurse in charge of the clinic Jane Olum said: “Yes, we get a lot of pneumonia, in different forms, some mild that can be treated and patient discharged and others very serious, and now I do not know where they will go.”
In a previous interview, Dr Adetifa clarified that a cough accompanied with difficulty in breathing and lower chest wall indrawing is a case of severe pneumonia.
But there is also severe pneumonia when the child presents one of the “danger signs” like inability to drink, seizures, altered consciousness, head nodding, and baby turning blue due to lack of oxygen.
In this case, Dr Agweyu explained, there would be a need for intensive care equipment: it is estimated that more than 80 percent of hospitals in Kenya do not have them.
While there have never been follow up studies on patients in Kenya, there are some in South Africa that have shown that deprivation of oxygen to the brain in some severe cases on Pneumonia have impacted negatively on the cognitive abilities even if the child survives.
Dr Agweyu added said “maybe the child would have grown up to be an athlete but a lung injury because they did not get intensive care on time robbed them of that opportunity”
Even with the best intentions, pneumonia has changed over the years, and yet the perception and treatment guidelines have not.
Pneumonia first appeared in the Kenyan policy documents for health in the late 80s.
After Kenya gained Independence, the census and household surveys showed a lot of neglected tropical diseases that have since been put under control such as aAnthrax, and bilharzia as a cause of death and disease in children.
It was always thought that only bacteria cause pneumonia.
Now, a three-decade study that was published this year showed that 60 percent of all the pneumonia is caused by viruses. The million-dollar Pneumonia Etiology Research for Child Health Study (PERCH) was conducted in Kenya and six other countries considered to be “high burden” for pneumonia, and found that viruses caused most (61 percent) of the severe pneumonia cases.
The respiratory syncytial virus (RSV) was the leading pathogen (31 percent) at all sites in all the 30 pathogens.
Bacteria was only responsible 27 percent of pneumonia.
DEEP IN THE LUNGS
That bacteria and these many viruses cause the disease, and the fact that these microorganisms lodge themselves deep within the lungs makes healthcare workers struggle to diagnose pneumonia.
Dr Agweyu who participated in the PERCH study told Business Daily that in certain cases, pneumonia that starts by viruses worsen to include bacterial complications.
The virus, he said, weakens the mucus-like cover in the lungs and this makes it easy for the bacteria to invade the child’s lungs. When the healthcare worker does make the diagnosis, there is also the complexity of how they categorise those patients according to the Ministry of Health guidelines.
The country has revised its World Health Organisation-approved guidelines on treating pneumonia after more than three decades but now experts are fearing the changes may lock many children out of much needed medical attention.
The new guidelines moved down the key physical sign previously used to identify severe pneumonia cases — whether the child’s lower chest wall was drawn in as they breathe — and made it be for non-severe pneumonia.
Non-severe case is considered an outpatient problem where the child is given oral antibiotics and discharged.
But Kemri researchers and another paediatrician from London School of Hygiene and Tropical Medicine Kim Mulholland expressed concern over WHO’s simplification of managing children with pneumonia into those two categories of “low risk” to be treated at home and “high risk” to be treated in hospital.
NEW GUIDELINES
Prof Mulholland and her Kenyan colleagues analysed data of 16,031 children sick of pneumonia in 14 of Kenya’s county hospitals before the new guidelines were formally rolled out. They found that five percent of these children (832) died.
Nearly two out of five of the kids that died (39 percent) had indrawing of the lower chest, and would, therefore, have been classified as “not severe” in these new guidelines.
Prof Mulholland explained that these changes made it easy to train health workers but their study needed a more nuanced approach. She said: “The numbers show that some of those with the “low risk” tag actually fall somewhere between low risk and high risk, an “unrecognised intermediate severity.”
The Ministry of Health had not responded to our questions by the time we were going to press.
Unlock a world of exclusive content today!Unlock a world of exclusive content today!