In December 2018, Kenya rolled out a pilot for a Universal Healthcare Coverage (UHC) targeting to provide quality and affordable health care to all by 2022.
Kisumu, Nyeri, Machakos and Isiolo are the pilot regions where an estimated 3.2 million are targeted for coverage before it is rolled out to the other 43 counties.
The four counties are scheduled to get a Sh3.17 billion conditional grant with each devolved unit getting Sh800 million. The counties will match that by their own investment and 80 per cent of the money will cater for drugs and basic medical equipment.
In his Agenda Four plan, President Uhuru Kenyatta indicated that a total of Sh44.6 billion had been set aside for UHC.
But with perennial under-funding of healthcare in Kenya, some reviews are a study in pessimism about the success of the campaign.
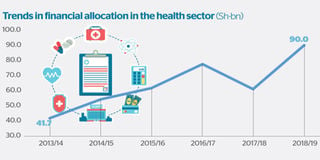
Although the value of health care financing in Kenya has improved in the past five years from Sh41.7 billion in 2013/14 to Sh90 billion in 2018/19, a report by the United Nations SDG Partnership Platform and Aavishkaar-Intellecap Group cautioned that that is not enough given the country’s reliance on external partners for monetary support.
“In the recent past, Kenya has experienced positive economic growth and become a lower middle-Income country; thus, the country is set to move progressively from external donor financing for health towards domestic funding,” the report said.
“For this to happen, Kenya must now start planning for the challenge of replacing the current external partner investments with internal resources from national and county governments and the private sector.”
Public healthcare in Kenya has customarily been financed by the State and donor agencies through grants and related funding.
It is primarily extended through subsidies and insurance schemes.
Kenya has also adopted the traditional approaches like National Health Insurance Fund (NHIF) to improve access to health services at the grassroots.
While the increase of total health expenditure of the government in Kenya is approximately 80 percent, the percentage of health care spending against the total State spending has hovered around 2.5 per cent over the period.
Counties expenditure on health as a proportion to the overall county government spending also rose from 5.26 percent (2013-14) to 19.28 per cent (2016-17).
“Health expenditures at national and county governments are on an increasing trend in absolute terms, but are stagnant in real terms at an average of five per cent of total government expenditures and 20 per cent for county expenditures,” says the report.
SDG Partnership and Intellecap Group, however, said research shows that four out of every five Kenyans have no access to medical insurance — throwing a challenge to Kenya of finding alternative financing for this crucial sector.
“There is an urgent need to look beyond the traditional approaches to health financing and identify ways to engage private sector, attract private capital and reduce dependency on already drying donor funding,” they said. Donor spending in Kenya’s healthcare sector has decreased significantly between 2010 and 2016.
A significant share of donor funding is for key programmes such HIV/Aids, TB, malaria, reproductive health and immunisation and thus the need for innovative financing.
Estimates showed that Kenya’s funding need for HIV, TB and Malaria alone would total Sh84 billion annually between 2019 and 2022, excluding health provider and infrastructure costs funded by government.
“Where the government should significantly increase its budgets for health to deliver on the country’s ambition to realise UHC, it should also tap into other sources of financing to optimise the existing resources and bridge critical gaps,” the SDG Partnership and Aavishkaar-Intellecap said.
Kenya, the report says, has the option to finance its healthcare through levies by, for example, taxing airline tickets, air travel being a luxury good.
Its also suggests the introduction of a telecoms levy for mobile phone subscribers to pay slightly more for mobile data and voice to potentially generate resources to support UHC.
“An estimated $122.5 million (Sh12.5 billion) is transacted daily in the form of mobile money transactions. By contributing roughly one percent on a graduated scale, Kenya can easily raise $1.2 million (Sh125 million) daily to finance UHC,” the report said.
Sin tax on goods such as tobacco and alcohol is also on the list of areas that would generate the budget considering their impact on consumers.
“A cess tax levied on tourists viewing Kenya’s wildlife and related tourism and recreational services. The total contribution of travel and tourism alone to Kenyan GDP was Sh769.1 billion or 9.7 percent of GDP in 2017, thus showing tremendous potential to support specific healthcare services in Kenya,” the partnership added.
Additionally, the partnership said, Kenya should consider imposing a Corporate Social Responsibility(CSR) levy on high net worth companies to finance its healthcare.
Kenya in June 2018 increase excise duty on mobile money transfers from 10 percent to 12 percent and a 0.05 percent excise duty on bank transfers of Sh500,000 or more. Taxing sugary and alcoholic beverages was also proposed but the idea did not see the light of day.
“The flipside of such taxes is that the tax impacts are usually passed on directly to consumers, increasing the costs of these products or services. This may reduce demand positively (for example, alcohol) or may increase the cost of living for those who can least afford the additional taxes,” the SDG Partnership and Aavishkaar-Intellecap warned.
Besides levies in health care financing, the group says Kenya may consider Social Impact Bonds (SIBs) and Developmental Impact Bonds (DIBs) which can improve the efficiency of government health care spending at the county as well as national levels.
This model has proved a success in Israel, India, Mozambique and Cameroon.
These innovative financing models help to fund health care through contracts where private investors provide upfront flexible funding to healthcare providers and outcome funders (usually government in case of social impact bonds and development finance institutions in case of development impact bonds) repay these investors based on the healthcare outcomes achieved by those who receive the services.
The SDG Partnership and Aavishkaar-Intellecap said the bonds would help finance child and maternal health components of the UHC.
The Division of Reproductive Health (DRH) is one of four units in the Department of Family Health, within the Ministry of Health (MOH) that works with partners in Kenya to reduce the high rates of maternal, neonatal and child morbidity and mortality and to help achieve the child and maternal health.
“A SIB/ DIB structure may be explored in this, which will improve effectiveness of the nationally envisaged reproductive health programme” the partners said.
Further, the group proposes the adoption of a Community Based Health Insurance(CBHI) schemes, which have been successful in Rwanda, Nigeria and Ghana to back up the implementation of UHC.
CBHI entails the protection of low-income people against specific perils in exchange for regular premium payments proportionate to the likelihood and cost of the risk involved. These are community-managed insurance schemes which are designed to help members manage financial risks associated and vulnerability associated with unexpected healthcare costs.
While there have been some experiments around CBHI schemes in Kenya such as the Chogoria Hospital Insurance Scheme, it has not been adopted at a large scale in the country.
Analysts said community participation is important to the success of a community-based health insurance scheme and also underwriting of the initial losses by the government can help the scheme set low rates at the beginning but may also give a false sense of affordability to the potential clients.
Hence the schemes can be sustainable in the long term only if serious attention is paid to their design and management.
“The premiums should also be reviewed at periodic intervals to ensure relevance and chargeability as per paying capacity,” the SDG Partnership and Aavishkaar-Intellecap observed in their report.
“Technology can also be leveraged to make CBHIs more robust, transparent, efficient and scalable,” it said.
“Also, it will be critical to align CBHI to the existing NHIF for long term sustainability. CBHIs is a way of ensuring those who are currently unemployed and cannot afford NHIF premiums are also provided adequate health coverage. It can act as a bridge between NHIF and the unemployed communities. Over a period of time these CBHIs can be aligned and merged into NHIF.”
The group says Kenya could also consider Advance Market Commitment (AMC) model to stimulate investment for its UHC.
Pharmaceutical and Diagnostic companies have long been reluctant to invest in producing new vaccines, drugs and diagnostics for the developing world because they have little prospect of earning an attractive return.
“One way to stimulate such investment is the use of an advance market commitment, an innovative financing programme that guarantees manufacturers a long-term market,” the partnership said.
Under this arrangement, international donors pay a premium for initial doses sold to developing countries. In exchange, companies agree to continue supplying the vaccine, drug or the diagnostic device (along with the consumable) over the longer term at more sustainable prices.
The global vaccine alliance, GAVI, has been working with Kenya in immunisation and health development since 2001 with $479 million (Sh48 billion) disbursed as by end of 2018.
“However, similar approaches could be applied to other therapeutic areas and product adaptations for low resource settings such as heat stable therapies or product and packaging redesign to align with how low income consumers purchase medicines,” the SDG Partnership and Aavishkaar-Intellecap said.
Further, the team says Kenya may need to explore Asset Lease Financing (ALF) in primary health care. While there has been some initiatives taken by the government to ensure the medical facilities are equipped with requisite devices and equipment in Kenya, the model has so far not been explored from the perspective of sole support and providing equipment and devices for health care.
“The model can be adopted for procurement of high cost laboratory equipment like GeneXpert, CD4 Analysers, X-ray machines at the county as well as the national level,” the group said.
The methods can also be leveraged to procure ambulances for primary care and maternal and child health service delivery.
Dental equipment can also be leased under this arrangement reduce the financial burden on the government.
“It can also be used for technology such as EMR or telemedicine equipment linked to outcome/adoption based payments, which ensure that the provider trains, upgrades, maintains the equipment and staff..., which are often problems with technology purchased once and rarely maintained or well-used.”
Unlock a world of exclusive content today!Unlock a world of exclusive content today!